

In our previous post, we explored how counties and public health departments can facilitate effective stakeholder engagement and community planning throughout the Behavioral Health Services Act (BHSA) transition. As the fifth installment in our BHSA Transition Guide series, we turn to another core pillar: strengthened statewide oversight and accountability.
Compliance under BHSA includes structured requirements for planning, service delivery, monitoring, and oversight for counties and funded providers, as well as critical milestones. Compared to the preceding Mental Health Services Act (MHSA), BHSA tightens expectations regarding performance, reporting, and the use of funds, with direct fiscal consequences.
This post addresses:
- How BHSA compliance differs from MHSA
- What happens when counties fall out of compliance
- What BHSA compliance review process requires of counties
- Why evaluators and external partners play a critical role in risk mitigation
By July 2026, all counties must fully transition to the new BHSA framework. As always, EVALCORP remains committed to helping our county partners navigate this transition thoughtfully and strategically, ensuring alignment with state expectations while addressing local behavioral health needs. There are several key BHSA deadlines over the next four years, and we are here to support you at each step of the process.
BHSA vs. MHSA Compliance
One of the central goals of California’s Behavioral Health Transformation is to increase accountability for publicly funded, county-administered behavioral health services. Under BHSA, compliance is no longer just about spending funds in allowable categories; it is about demonstrating outcomes, fidelity to priorities, and continuous oversight.
BHSA reshapes county expectations around data transparency and performance. Under BHSA, counties must:
- Prepare Integrated Plans (IPs) every three years that encompass all local behavioral health funding streams.
- Submit annual Behavioral Health Outcomes, Accountability, and Transparency Reports (BHOATR) with aligned fiscal, service, and outcomes metrics.
- Undertake a Community Planning Process (CPP) that allows clients, families, and community partners to inform priorities and planned activities directly.
Together, these requirements standardize reporting across counties and strengthen comparability, accountability, and oversight across funding categories. Key differences between MHSA and BHSA compliance frameworks are summarized in Table 1 below.
Table 1.

BHSA Sanctions and Non-Compliance
If the Department of Health Care Services (DHCS) determines that a county is out of compliance with BHSA requirements, as outlined in the state law, the Policy Manual, and the County Performance Contract, DHCS may pursue various enforcement actions. These include:
- Administrative sanctions: DHCS can require counties to submit corrective action plans (CAPs), or impose DHCS‑defined CAPs when it finds BHSA noncompliance. CAP rules align with Medi-Cal CAP practices. DHCS may also direct a county to revise its IP or Annual Update (AU) when stakeholder engagement, required components, or other statutory requirements are not met.
- Monetary tools: For significant or repeated violations, DHCS may impose temporary funding withholds or monetary sanctions. DHCS can withhold up to 25% of a county’s monthly allocations from the Behavioral Health Services Fund (BHSF) until it has collected the full sanction amount.
In addition, DHCS operates a related quality enforcement framework that imposes monetary penalties when behavioral health plans fail to meet minimum performance thresholds for specified quality measures. Sanction amounts are scaled to county size. Grounds for enforcement may include failure to comply with CPP requirements, missed IP or AU deadlines, misuse or underexpenditure of funds, or unresolved prior CAP findings under either BHSA or MHSA.
While monetary withholds or sanctions are in effect, counties remain responsible for meeting all BHSA program requirements unless otherwise directed by DHCS. The state generally intends to begin with temporary withholds and escalate enforcement only in cases of severe or persistent noncompliance.
Importantly, unlike Medi-Cal sanctions, BHSA monetary penalties are returned to the county upon compliance. Counties are also afforded formal notice and appeal rights, including the ability to request a hearing within specified timeframes following a sanction notice.
State Compliance Review Processes
According to the BHSA County Policy Manual, Module 4, DHCS will conduct periodic reviews to assess each county’s compliance with BHSA program requirements, as it currently does for MHSA and other county-administered behavioral health programs.
Frequency and Timing
- Routine BHSA compliance reviews are expected to begin no earlier than SFY 2027–2028, with the first review period covering SFY 2026–2027 (the first program year under the 2026 Integrated Plan)
- DHCS anticipates conducting annual compliance reviews, with an onsite review occurring at least once every three years
- DHCS may also initiate targeted ad hoc reviews at any time if serious or urgent compliance concerns arise
In various sections of the IP and AU templates, DHCS has included space for counties to disclose implementation challenges or concerns related to specific requirements under BHSA, as well as to other programs and funding sources managed by counties. These self-disclosures are optional, and DHCS does not interpret them as automatic admissions of noncompliance. Instead, DHCS aims to collect data on common concerns to guide technical assistance efforts.
Compliance Review Process
The BHSA compliance review process is modeled after Medi-Cal compliance reviews outlined in Behavioral Health Information Notice (BHIN) 23-044 and includes four phases:
1. Review Preparation
- Pre-review planning
- County document submissions
- DHCS desk review of materials
2. Compliance Review
- Conducted onsite or virtually
- Focuses on program implementation, documentation, and adherence to BHSA requirements
3. Post-Review Evidence & Exit Process
- County opportunity to respond to draft findings
- Additional documentation or clarification may be submitted
4. Findings Report
- DHCS issues formal report
- Identifies areas of compliance and noncompliance
Includes any recommended or required corrective actions
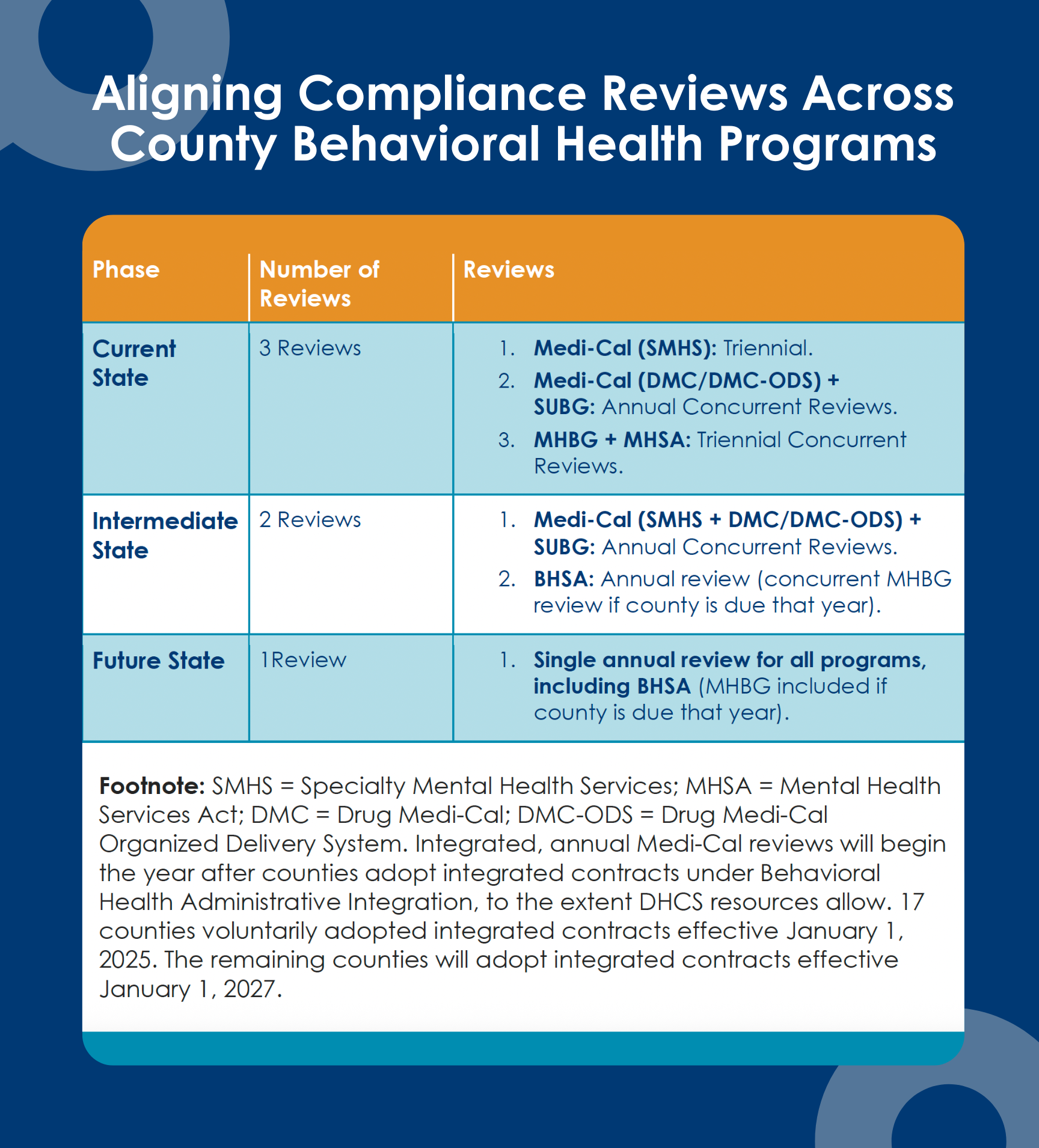
To reduce administrative burden, DHCS intends to align BHSA compliance reviews with other county behavioral health reviews, including:
- Medi-Cal Specialty Mental Health Services (SMHS)
- Drug Medi-Cal (DMC) and DMC-ODS
- Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG)
- Community Mental Health Services Block Grant (MHBG)
DHCS is considering conducting a single compliance review for each county annually, either virtually or onsite. This concurrent review would assess both BHSA and the other county-administered programs listed above simultaneously. By consolidating these reviews, DHCS aims to enhance efficiency at both the county and state levels by avoiding duplicate requests for pre-review document submissions, aligning similar requirements across programs where feasible, and streamlining the review process to the extent possible. See Table 2 below.
Table 2
The Role of Evaluator Support
Given the scope and complexity of BHSA requirements, many counties are increasingly recognizing the value of independent evaluators and compliance partners to support a successful transition.
While DHCS does not anticipate implementing formal monetary sanctions until a later phase of BHSA implementation—currently expected around the next Integrated Plan cycle—and continues to develop additional guidance, data tools, and monitoring supports through DHCS and CalMHSA, early preparation remains critical.
Support from a program evaluation consultant can help counties to:
- Systematically assess current data, reporting, and monitoring capabilities relative to BHSA’s future performance and accountability standards; and
- Build internal capacity to track, analyze, and report required metrics consistently and defensibly, reducing risk as full enforcement and performance expectations come online.
Engaging evaluation and compliance expertise early allows counties to move from reactive compliance toward proactive system readiness—easing the eventual transition to full BHSA accountability while supporting continuous quality improvement.
How EVALCORP Can Help with BHSA Compliance
Our BHSA Compliance and Integration Workgroup is actively tracking these developments and providing hands-on support to counties across California. From community engagement strategy development to data system design and outcome reporting, EVALCORP is ready to support you through every stage of the transition. Please contact us if you’d like to learn more.